

 |
| PML |
Progressive multifocal leukoencephalopathy (PML) has been reported as a serious adverse event affecting 1/1,000 to 1/100 Natalizumab (Nz) -treated patients with 20% of the fatal issue.
Three factors that are known to increase the risk of PML in natalizumab-treated patients have been identified: be the principal the presence of anti-JCV antibodies, the other ones, it is longer treatment duration, especially beyond 2 years and prior treatment with an immunosuppressant (e.g., azathioprine, cyclophosphamide, mitoxantrone, methotrexate, mycophenolate mofetil). either has used an immunosuppressant before starting Tysabri, or have not used immunosuppressants and have a high JC virus antibody index.
The following is Biogen's quarterly update; if you are not a healthcare professional (HCP) you shouldn't be reading the document *.
• As of February 28, 2017, approximately 167,300 patients received natalizumab in the postmarketing setting worldwide
• As of March 6, 2017, there have been 714 confirmed PML cases (711 MS, 3 Crohn’s Disease), (199 USA, 448 UE, 67 rest of the world). Based on follow-up data for at least 6 months after PML diagnosis, 77% patients were alive with varying levels of disability; 23% of patients have died. The duration of natalizumab dosing prior to PML diagnosis ranged from 8 to 134 doses. The mean duration of natalizumab dosing at the time of PML diagnosis was approximately 48 months (Biogen website)
• (Biogen website, if you are not an HCP you shouldn't be reading the document *) at 2015, at which time 566 PML cases had been confirmed. Of these 566 patients 62 (11.0%) were identified as asymptomatic (defined as patients who had no clinical symptoms of PML, but had MRI findings consistent with PML and detectable JC virus DNA in the central nervous system (CNS)) and 504 (89.0%) were identified as symptomatic at PML diagnosis. 95.2% of asymptomatic patients and 74.2% of symptomatic patients were alive. We analyzed all available data on functional disability in asymptomatic and symptomatic PML cases (EDSS and Karnofsky scores) and observed that asymptomatic PML patients appeared to have a less functional disability than did symptomatic patients prior to PML diagnosis, at diagnosis, and post diagnosis.
• Recent studies (Prosperini et al) suggest that early detection and treatment of PML when the disease is asymptomatic (is still in the initial stages and shows no symptoms) may improve patients’ outcomes. (and the data of Biogen, confirm that ¡¡¡)
This rise the question, what to do, with the 80% of survivors of PML, with previously natalizumab treatment?
Natalizumab-PML survivors with subsequent MS treatment: Clinico-radiologic outcome
- Elisabeth Maillart, MD,
- Jean-Sebastien Vidal, MD, PhD,
- David Brassat, MD, PhD,
- Bruno Stankoff, MD, PhD,
- Agnès Fromont, MD, PhD,
- Jérôme de Sèze, MD, PhD,
- Frédéric Taithe, MD, PhD,
- Pierre Clavelou, MD, PhD,
- Bertrand Bourre, MD,
- Valérie Delvaux, MD, PhD,
- Audrey Rico, MD, PhD,
- Pierre Labauge, MD, PhD,
- Ayman Tourbah, MD, PhD,
- Christine Lebrun, MD, PhD,
- Jean Pelletier, MD, PhD,
- Thibault Moreau, MD, PhD,
- Céline Louapre, MD, PhD,
- Catherine Lubetzki, MD, PhD and
- Caroline Papeix, MD
- On behalf of SFSE
Published online April 14, 2017
doi: http:/ / dx. doi. org/ 10. 1212/ NXI. 0000000000000346Neurol Neuroimmunol Neuroinflamm May 2017 vol. 4 no. 3 e346
This paper reported an observational multicenter, retrospective cohort of 23 patients with MS surviving after Nz-PML.
They found:
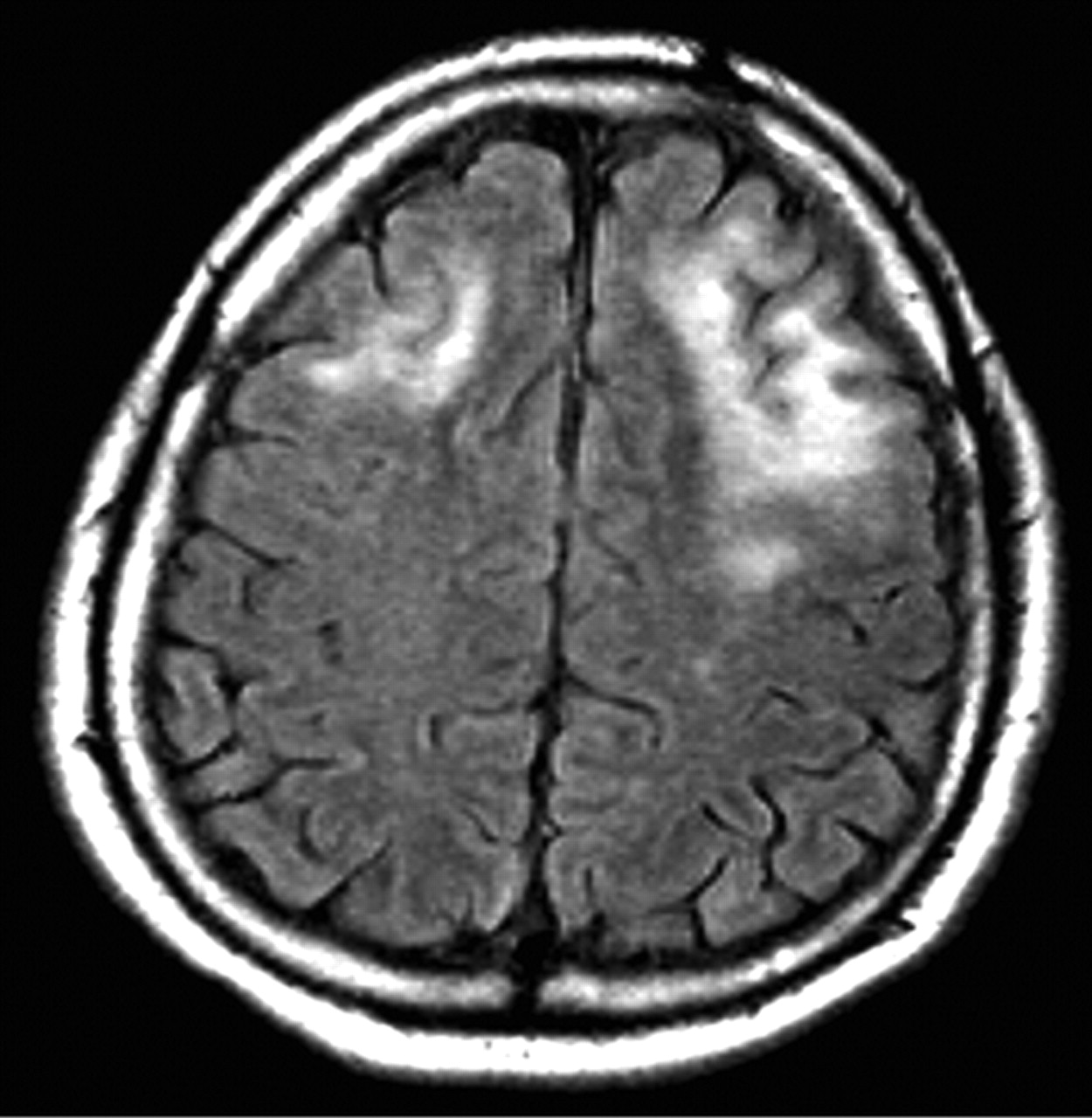
- PML occurred on average after 45.9 (14.7) infusions, i.e., 3.86 years (1.58). The most frequent initial PML symptoms were limb weakness (43.5%) and cerebellar ataxia (30.4%). MRI revealed a unique frontal lesion in 36.4% of cases. Multifocal lesions were observed in 31.8% of cases, and gadolinium enhancement was detected in 54.5% of cases at Nz-PML diagnosis.
- In patients with highly active MS, the reappearance of disease activity after Nz discontinuation seems faster and more severe than in patients with low activity preceding Nz treatment.
- Fingolimod was the DMT use more frequently in this cohort to treat patients after Nz-PML with good results.
- It must take into consideration: the small numbers of patients and the retrospective and multicenter design, but give us data about what happen with these patients.

Timeline of subsequent MS treatments, after Nz-PML for each patient of the cohort The zero on the x-axis represents the diagnosis of Nz-PML. Black line: washout period after natalizumab cessation without any MS disease-modifying therapy. Blue line: interferon β. Red line: glatiramer acetate. Peach line: dimethyl fumarate. Green line: fingolimod. Asterisk: one clinical relapse. Circle: new MS lesions on brain MRI. Cross: intolerance of the treatment. MS = multiple sclerosis; Nz-PML = natalizumab-related progressive multifocal leukoencephalopathy.
Starting DMT ( natalizumab) in a patient with MS, keep the following considerations in mind:
For the neurologist should follow these recommendations: (European Guidelines)
• Before starting treatment with Tysabri, patients and carers should be advised about the risk of PML. Patients should be instructed to seek medical advice if they think their disease is getting worse, or if they notice any new or unusual symptoms.
• Before starting treatment, a baseline MRI should be available (usually within 3 months) as a reference, and a baseline anti-JCV antibody test should be performed to support PML risk stratification.
• During treatment with Tysabri, patients should be monitored at regular intervals for signs and symptoms of new neurological dysfunction, and a full brain MRI should be performed at least once a year for the duration of treatment.
• For patients at higher risk of PML, more frequent MRIs (e.g. every 3-6 months) using an abbreviated protocol (e.g. FLAIR, T2-weighted and DW imaging) should be considered, as earlier detection of PML in asymptomatic patients is associated with improved PML outcomes.
• PML should be considered in the differential diagnosis of any patient presenting with neurological symptoms and/or new brain lesions on MRI. Cases of asymptomatic PML based on MRI and positive JC virus DNA in the CSF have been reported.
• If PML is suspected, the MRI protocol should be extended to include contrast-enhanced T1-weighted imaging and testing of CSF for the presence of JC virus DNA using ultrasensitive PCR should be considered.
• If PML is suspected at any time, treatment with Tysabri must be stopped until PML has been excluded.
• Anti-JC virus antibody testing should be done every 6 months in antibody-negative patients. Patients who have low index values and no history of prior immunosuppressant use should also be retested every 6 months once they reach the 2-year treatment point.
• After 2 years of treatment, patients should be informed again about the risk of PML with Tysabri.
• Patients and carers should be advised to continue to be vigilant about the risk of PML for up to 6 months following discontinuation of Tysabri.
*The context of the information that refers to the professional health personnel, is applied since the information provided by BIOGEN, has to be analyzed by its individual health professional, applied to his own evolution of the patient, clinical characteristics and evolution of the disease, and lack of understanding of it would lead to a misapplied concept. Since multiple sclerosis is a complex disease, the knowledge of the treatments and complications derived from it must be seen in an integral way and in risk - benefit contexts, totally individualized.
*The context of the information that refers to the professional health personnel, is applied since the information provided by BIOGEN, has to be analyzed by its individual health professional, applied to his own evolution of the patient, clinical characteristics and evolution of the disease, and lack of understanding of it would lead to a misapplied concept. Since multiple sclerosis is a complex disease, the knowledge of the treatments and complications derived from it must be seen in an integral way and in risk - benefit contexts, totally individualized.
 |
| AImmunohistochemical detection of JC virus protein (brown stained) in a brain biopsy (infected glial cells in PML) |
La leucoencefalopatía multifocal progresiva (PML) es una enfermedad desmielinizante devastadora con morbilidad y mortalidad significativas altas y sin terapias eficaces en la actualidad. El agente etiológico de la PML es un pequeño y omnipresente polyomavirus, el virus JC (JCV, también conocido como JCPyV), para el cual al menos el 50% de la población general adulta es seropositiva. PML es la resultante de la replicación del virus JC dentro de oligodendrocitos y astrocitos, lo que conduce a la muerte de oligodendrocitos y la desmielinización. Este virus es muy común en la población general y normalmente es inofensivo; Sin embargo, puede conducir a PML en personas cuyo sistema inmunológico está debilitado. Los síntomas más comunes de PML son una debilidad progresiva, problemas de habla y comunicación, alteración visual y, a veces, cambios en el estado de ánimo o del comportamiento. PML es una condición muy grave que puede resultar en discapacidad grave o la muerte.
La leucoencefalopatía multifocal progresiva (PML) ha sido reportada como un evento adverso grave que afecta a 1 / 1.000 a 1/100 pacientes tratados con Natalizumab (Nz), con el 20% de mortalidad.
Se han identificado tres factores que se sabe que aumentan el riesgo de PML en pacientes tratados con natalizumab: siendo el principal la presencia de anticuerpos anti-JCV, los otros, es la duración del tratamiento, especialmente más allá de 2 años y el tratamiento previo con un Inmunosupresor (por ejemplo, azatioprina, ciclofosfamida, mitoxantrona, metotrexato, micofenolato mofetil). O bien ha utilizado un inmunosupresor antes de iniciar Tysabri, o no ha utilizado inmunosupresores y tiene un alto índice de anticuerpos del virus JC.
La siguiente es la actualización trimestral de Biogen; Si usted no es un profesional de la salud (HCP) no debe estar leyendo el documento*.
• A partir del 28 de febrero de 2017, aproximadamente 167.300 pacientes recibieron natalizumab en el mercado postcomercialización en todo el mundo
• Al 6 de marzo de 2017, se han confirmado 714 casos de PML (711 MS, 3 de Crohn), (199 USA, 448 UE, 67 resto del mundo). Sobre la base de datos de seguimiento durante al menos 6 meses después del diagnóstico de PML, el 77% de los pacientes estaban vivos con diferentes niveles de discapacidad; El 23% de los pacientes han fallecido. La duración de la dosis de natalizumab antes del diagnóstico de PML varió de 8 a 134 dosis. La duración media de la dosis de natalizumab en el momento del diagnóstico de PML fue de aproximadamente 48 meses (sitio web de Biogen).
• (Sitio web de Biogen, si usted no es un HCP que no debería leer el documento*) en 2015, momento en el que se habían confirmado 566 casos de PML. De estos 566 pacientes, 62 (11,0%) fueron identificados como asintomáticos (definidos como pacientes sin síntomas clínicos de PML, pero con resonancia magnética (RM), consistente con PML y ADN detectable del virus JC en el sistema nervioso central) y 504 (89,0 %) fueron identificados como sintomáticos en el diagnóstico de PML. El 95,2% de los pacientes asintomáticos y el 74,2% de los pacientes sintomáticos estaban vivos. Se analizaron todos los datos disponibles sobre la discapacidad funcional en los casos asintomáticos y sintomáticos de PML (puntuaciones de EDSS y Karnofsky) y observó que los pacientes asintomáticos de PML parecían tener una discapacidad menor que los pacientes sintomáticos antes del diagnóstico de PML.
• Estudios recientes (Prosperini et al) Sugieren que la detección temprana y el tratamiento de la PML cuando la enfermedad es asintomática (todavía está en las etapas iniciales y no muestra síntomas) puede mejorar los resultados de los pacientes. (Y los datos de Biogen, lo confirma ¡¡¡)
Todo esto genera la pregunta, ¿qué hacer, con el 80% de los sobrevivientes de PML, con tratamiento previamente de natalizumab?
Natalizumab-PML survivors with subsequent MS treatment: Clinico-radiologic outcome
- Elisabeth Maillart, MD,
- Jean-Sebastien Vidal, MD, PhD,
- David Brassat, MD, PhD,
- Bruno Stankoff, MD, PhD,
- Agnès Fromont, MD, PhD,
- Jérôme de Sèze, MD, PhD,
- Frédéric Taithe, MD, PhD,
- Pierre Clavelou, MD, PhD,
- Bertrand Bourre, MD,
- Valérie Delvaux, MD, PhD,
- Audrey Rico, MD, PhD,
- Pierre Labauge, MD, PhD,
- Ayman Tourbah, MD, PhD,
- Christine Lebrun, MD, PhD,
- Jean Pelletier, MD, PhD,
- Thibault Moreau, MD, PhD,
- Céline Louapre, MD, PhD,
- Catherine Lubetzki, MD, PhD and
- Caroline Papeix, MD
- On behalf of SFSE
Published online April 14, 2017
doi: http:/ / dx. doi. org/ 10. 1212/ NXI. 0000000000000346Neurol Neuroimmunol Neuroinflamm May 2017 vol. 4 no. 3 e346
Este trabajo informó de una observación multicéntrica , cohorte retrospectiva de 23 pacientes con EM que sobreviven después de Nz-PML.
Ellos encontraron:
- PML ocurrió en promedio después de 45,9 (14,7) infusiones, es decir, 3,86 años (1,58). Los síntomas iniciales más frecuentes de PML fueron debilidad de las extremidades (43,5%) y ataxia cerebelosa (30,4%). La RM mostró una lesión frontal única en el 36,4% de los casos. Se observaron lesiones multifocales en el 31,8% de los casos y se detectó realce de gadolinio en el 54,5% de los casos con diagnóstico de Nz-PML.
- En pacientes con EM altamente activa, la reaparición de la actividad de la enfermedad después de la interrupción de Nz parece más rápidamente y con mayor severidad, que, en pacientes con baja actividad, anterior al tratamiento con Nz
- Fingolimod fue DMT de mayor frecuencia de utilización en esta cohorte para tratar a los pacientes después de Nz-PML con buenos resultados.
- Debe tener en cuenta: el pequeño número de pacientes y el diseño retrospectivo y multicéntrico, pero nos dan datos sobre lo que sucede con estos pacientes.
Al comenzar el DMT (natalizumab) en un paciente con EM, tenga en cuenta las siguientes consideraciones:
Para el neurólogo debe seguir estas recomendaciones: (Directrices europeas)
• Antes de iniciar el tratamiento con Tysabri, los pacientes y los cuidadores deben ser informados sobre el riesgo de PML. Los pacientes deben ser instruidos para buscar consejo médico si piensan que su enfermedad está empeorando, o si notan cualquier síntoma nuevo o inusual.
• Antes de comenzar el tratamiento, debe estar disponible una resonancia magnética basal (generalmente en un plazo de 3 meses) y se debe realizar una prueba basal de anticuerpos anti-JCV para apoyar la estratificación del riesgo de PML.
• Durante el tratamiento con Tysabri, los pacientes deben ser monitoreados a intervalos regulares para detectar signos y síntomas de nueva disfunción neurológica, y se debe realizar una resonancia magnética cerebral completa al menos una vez al año durante el tratamiento.
• Para pacientes con mayor riesgo de PML, se deben considerar RM más frecuentes (por ejemplo, cada 3-6 meses) utilizando un protocolo abreviado (por ejemplo, FLAIR, T2 y DW), ya que la detección temprana de PML en pacientes asintomáticos está asociada con resultados mejorados del PML.
• La PML debe ser considerada en el diagnóstico diferencial de cualquier paciente que presente síntomas neurológicos y / o nuevas lesiones cerebrales en la RM. Se han notificado casos de PML asintomática basados en la RM y el ADN del virus JC positivo en el LCR.
• Si se sospecha PML, el protocolo de MRI debe ampliarse para incluir imágenes de contraste ponderadas en T1 y pruebas de CSF para detectar la presencia de ADN del virus JC usando PCR ultrasensible.
• Si se sospecha PML en cualquier momento, el tratamiento con Tysabri debe detenerse hasta que se haya excluido la PML.
• La prueba de anticuerpos contra el virus JC debe realizarse cada 6 meses en pacientes con anticuerpos negativos. Los pacientes que tienen bajos valores de índice y sin antecedentes de uso previo de inmunosupresores también deben volver a ser examinados cada 6 meses una vez que alcanzan el punto de tratamiento de 2 años.
• Después de 2 años de tratamiento, los pacientes deben ser informados de nuevo sobre el riesgo de PML con Tysabri.
• A los pacientes y cuidadores se les debe aconsejar que sigan vigilantes sobre el riesgo de PML hasta 6 meses después de la interrupción de Tysabri.
* El contexto de la informacion que se refiere hacia el personal profesional de la salud , se aplica dado que la informacion aportada por BIOGEN, tiene que ser analizada por su profesional de salud en forma individual , aplicada a su propia evolucion , caracteristicas clinicas y evolucion de la enfermedad , y la falta de entendimiento de la misma llevaria a un concepto aplicado no apropiado . Siendo la Esclerosis Multiple una enfermedad compleja , el conocimiento de los tratamientos y complicaciones derivados de la misma , tienen que ser vistos en forma integral y en contextos de riesgo - beneficio, totalmente individualizados.

No hay comentarios:
Publicar un comentario